SIK KARŞILAŞILAN BİR OMUZ AĞRISI NEDENİ: ROTATOR KUF HASTALIĞI
It is the most common cause of shoulder pain in people over the age of thirty. Rotator cuff disease causes dull pain on the upper, front and outer surface of the shoulder. This pain characteristically increases with lying down at night and with shoulder movements. The likelihood of its occurrence increases with age, and pain and limitation may occur even in basic activities such as combing hair, moving your hand behind your back, or putting on something.
The ball-socket-shaped shoulder joint is formed by the meeting of the knob-shaped head of the arm bone and the shallow and flat socket of the shoulder blade. These parts that make up the shoulder joint are held together by loose ligaments and surrounded by a cover of muscles and tendons called the rotator cuff.
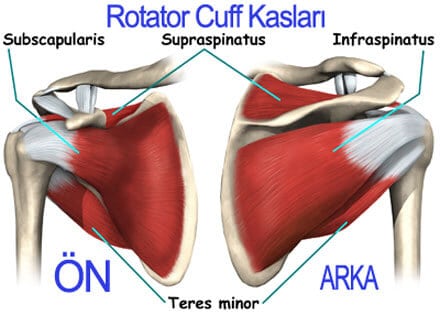
The rotator cuff consists of four muscles surrounding the shoulder joint (supraspinatus, infraspinatus, teres minor and subscapularis) and the tendons (hard tissue bands that connect muscles to bones) of these muscles that attach to the upper arm bone. These tendons attach to the upper arm bone and form a cuff surrounding the head of this bone. The rotator cuff not only helps the shoulder move in different directions, but also helps prevent shoulder dislocation by keeping the shoulder joint stable. Among these muscles, the supraspinatus allows the arm to be lifted to the side, while the infraspinatus and teres minor are responsible for moving the arm outwards and the subscapularis is responsible for moving the arm inwards. Repetitive activities and overuse can damage tendons, leading to pain and dysfunction. Rotator cuff disease of the shoulder is mostly caused by progressive wear or tear of the tendons over time and can cause disease conditions such as rotator cuff tendinitis or rotator cuff rupture. In this disease, any of the rotator cuff tendons can be injured, but the tendon of the supraspinatus muscle, which is the most important and sensitive component of this structure and is responsible for lifting the arm, is most frequently injured.
Rotator cuff tendinitis;
It usually occurs with repetitive reaching overhead, pushing, or lifting with the arm stretched and straight.
Rotator cuff rupture;
Rotator cuff tendons can be torn by major trauma (such as a fall, direct blow, rapid use of force, or accidents), a prolonged condition of chronic tendinitis, or a combination of both.
Risk factors;
-Age: The risk of rotator cuff injury increases with age. Tendon tears are common in people over the age of 60.
-Some professions: It is a disease that is very common among manual laborers and those whose jobs involve a lot of repetitive movements, and the risk of occurrence increases in some professions that frequently put their arms in overhead positions, such as wall painters, car mechanics, and carpenters.
-Sporting activities: Sports performed with repetitive activities in overhead positions such as basketball, tennis, swimming, golf, weightlifting, throwing, volleyball and gymnastics increase the risk of rotator cuff disease.
-Anatomical deformities of the shoulder joint: Deformities that predispose the rotator cuff muscles to compression increase the risk. It has been observed that factors such as improper position of the scapula, conditions related to instability or movement disorders, and genetic or familial predispositions increase the risk of rotator cuff disease. Symptoms: Shoulder pain; In this disease, pain is usually felt on the upper, front and outer surface of the shoulder and can spread from the outside of the arm to the elbow.
Night pain; It is common for the patient to have night pain and disrupt sleep when lying on his shoulder.
Pain and limitation with movement; There is a situation where shoulder movements such as reaching, pushing, pulling, lifting and placing above shoulder level aggravate the pain and prevent normal joint movements.
Weakness; In those with a rotator cuff tear, weakness may be felt in the arm during movements in certain directions.
Restriction in functions; There may be restrictions in daily living activities in the long term.
make a diagnosis
The diagnosis of this disease is based on a detailed history of the disease, the patient’s symptoms and the physician’s examination. After the examination, your physician may request radiological examinations such as x-ray, ultrasound and/or MRI to confirm the diagnosis and exclude other causes that may cause shoulder pain.
Treatment
Treatment of this disease focuses on reducing pain, preserving the range of motion of the shoulder joint, restoring range of motion if there is a limitation, and restoring shoulder functions by strengthening the muscles with decreased strength. In patients who do not use their shoulder joint less due to pain, this may cause shoulder movement to be further restricted, leading to a frozen shoulder condition in which movements are completely eliminated.
NON-SURGICAL TREATMENTS
Rest and activity modification: It is essential to avoid repetitive overhead activities, heavy lifting, or activities that increase symptoms. When the pain is severe, it is safe to keep the arm down in front of and near the body. During very painful periods, a shoulder strap can be tried for a short time, but it should be kept in mind that it may cause frozen shoulder.
Medication use: Painkillers and inflammation-reducing medications are used. For this purpose, non-steroidal (cortisone) inflammation-reducing drugs (NSAIDs) can be used by taking them orally and applying them externally on the shoulder joint (creams, gels, etc.). These drugs relieve pain in the short term. Additionally, nitroglycerin creams applied externally to the skin can be tried. For those with very severe pain, short-term opioid medications can be given.
Intra-articular injections: Apart from injections with a mixture of cortisone and local anesthetic, various injections such as hyaluronic acid, PRP, Prolotherapy can be used.
Physical therapy and rehabilitation practices:
In this context, heat applications such as cold and hot, laser, therapeutic ultrasound, electrical stimulation and electric current applications, iontophoresis, phonophoresis, acupuncture applications, kinesiotaping (taping), ESWT, massage and manual therapy applications are performed depending on the disease period. Exercises are of special importance in rehabilitation practices. Pendulum exercises prevent the development of frozen shoulder by stretching the tendons, so they are started very early following the onset of the disease or shoulder injection. There are many studies showing that a wide variety of exercise practices, such as joint range of motion, stretching, strengthening and endurance of the muscles around the shoulder, scapular stabilization and strengthening, accelerate recovery and eliminate restrictions in daily life activities and functions by gaining pain-free movement.
No more than mild pain should be felt during exercises. If it is felt, the number of repetitions and intensity of the exercise should be reduced. An exercise that causes too much pain should not be continued. In addition, pain after exercises should not last more than 24 hours.
SURGICAL TREATMENT:
In rotator cuff tendinitis It is essential to strive primarily for non-surgical treatments. In this disease, a surgical approach is required because non-surgical treatments, which are usually applied for 3-6 months, are ineffective or shoulder functions worsen despite the treatments.
In rotator cuff tears, treatment with a surgical approach is preferred for one or more full-thickness tears in young active patients. For non-full-thickness (partial) tears, non-surgical treatments are primarily applied unless the patient is older, less active, and has less pain. A wide variety of surgeries can be performed in rotator cuff tears, depending on the severity of the disease and the surgeon’s decision. In order for shoulder strength and functions to return to normal, it is optimal for the operation to be followed by physical therapy and rehabilitation practices.
course of the disease
Most patients with rotator cuff tendinitis experience pain relief and improved function with nonsurgical treatments for 6 to 12 weeks.
Prof. Dr. Belma Füsun Köseoğlu
FOR MORE INFORMATION;
1-Fahy K, Galvin R, Lewis J, Mc Creesh K. Exercise as effective as surgery in improving quality of life, disability, and pain for large to massive rotator cuff tears: A systematic review & meta-analysis. Musculoskelet Sci Pract. 2022 Oct;61:102597. doi: 10.1016/j.msksp.2022.102597. Epub 2022 Jun 10. PMID: 35724568.
2-Varacallo M, El Bitar Y, Mair SD. Rotator Cuff Tendonitis. 2023 Aug 4. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan–. PMID: 30335303.
3-Sciarretta FV, Moya D, List K. Current trends in rehabilitation of rotator cuff injuries. SICOT J. 2023;9:14. doi: 10.1051/sicotj/2023011. Epub 2023 May 23. PMID: 37222530; PMCID: PMC10208043.
4-May T, Garmel GM. Rotator Cuff Injury. 2023 Jun 26. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan–. PMID: 31613444.
5-Prabhakar A, Kanthalu Subramanian JN, Swathikaa P, Kumareswaran SI, Subramanian KN. Current concepts on management of cuff tear. J Clin Orthop Trauma. 2022 Feb 18;28:101808. doi: 10.1016/j.jcot.2022.101808. PMID: 35402155; PMCID: PMC8983388.
